Robotic McKeown Esophagectomy: Precision Management of Mid-Thoracic Esophageal Cancer
At our institution, we continuously strive to bring cutting-edge medical technology to the forefront of patient care. This month’s case profile highlights a significant clinical milestone: the successful surgical management of a 51-year-old male diagnosed with Carcinoma of the Mid-Thoracic Esophagus. By utilizing advanced robotic infrastructure, our multi-disciplinary surgical oncology team executed a highly complex three-stage procedure, offering an optimal oncological clearance and an accelerated recovery pathway.
Patient Profile & Clinical Presentation
| Age / Demographics | 51-Year-Old Male |
| Chief Complaints | Progressive dysphagia (difficulty swallowing) over 3 months, initially restricted to solids and subsequently progressing to liquids, associated with significant unintentional weight loss |
| Final Diagnosis | Biopsy and staging evaluation confirmed a localized Carcinoma of the Mid-Thoracic Esophagus |
The Clinical Challenge
The mid-thoracic esophagus resides within a highly restrictive and critical anatomical territory, bordered closely by major vital structures including the trachea, the descending thoracic aorta, and the main pulmonary vessels. Traditional open surgery requires a large thoracotomy (chest incision) alongside a substantial laparotomy (abdominal incision). These approaches are historically associated with intense post-operative pain, prolonged hospitalization, and heightened risks of severe respiratory complications.
To mitigate surgical trauma and execute a highly precise radical lymphadenectomy, our multi-disciplinary tumor board opted for a minimally invasive, Robotic-Assisted McKeown Three-Stage Esophagectomy.
Operative Spotlight: Three-Stage Reconstruction
The procedure was meticulously coordinated across three sequential phases, leveraging the high-definition 3D visualization and wristed instrumentation of the surgical robotic platform:
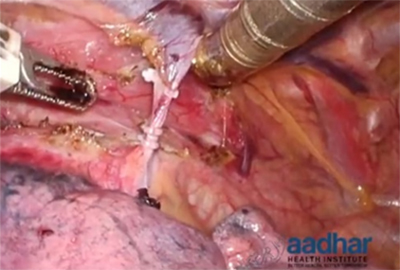
Phase 1: Thoracic Phase (Robotic-Assisted)
With the patient in a prone/semi-prone position, keyhole ports were utilized to dock the robotic system. The robot permitted precise dissection of the mid-thoracic esophagus cleanly away from the aorta and bronchial tree. A radical mediastinal lymphadenectomy was performed with absolute precision, safely preserving the delicate bilateral recurrent laryngeal nerves.
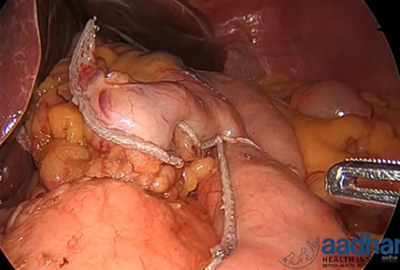
Phase 2: Abdominal Phase (Laparoscopic / Robotic)
The surgical field was moved to the abdomen to cleanly mobilize the stomach. A slender, vascularized gastric conduit (tube) was fashioned to serve as the structural replacement for the resected esophagus. Comprehensive radical abdominal lymph node clearance was simultaneously achieved.
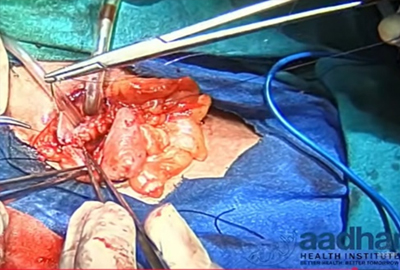
Phase 3: Cervical Phase (Neck Anastomosis)
A small incision was executed on the left side of the neck. The diseased segment of the esophagus was carefully extracted, and the newly prepared gastric conduit was pulled up smoothly through the posterior mediastinum into the cervical region. A precise, tension-free connection (anastomosis) was established between the healthy cervical esophagus and the new gastric tube.
Post-Operative Course & Complete Remission
Benefiting from the minimally invasive architecture of the robotic approach, the patient demonstrated an excellent recovery curve. Post-operative pain was minimal, requiring low-dose analgesia, which allowed for out-of-bed mobilization on Day 1. Trial Feed was started on Day 1 which was well tolerated by patient. ICD was removed on POD 4 , Patient was discharged on POD 5