Successful Management of Postoperative Hemorrhage Following Laparoscopic Common Bile Duct Exploration Requiring Angioembolization
A 73-year-old female with a history of laparoscopic cholecystectomy (3 years prior) presented with abdominal pain. MRCP demonstrated a 13 mm common bile duct (CBD) stone. She had previously undergone ERCP; however, the CBD stone persisted. There was no clinical or biochemical evidence of obstructive jaundice.
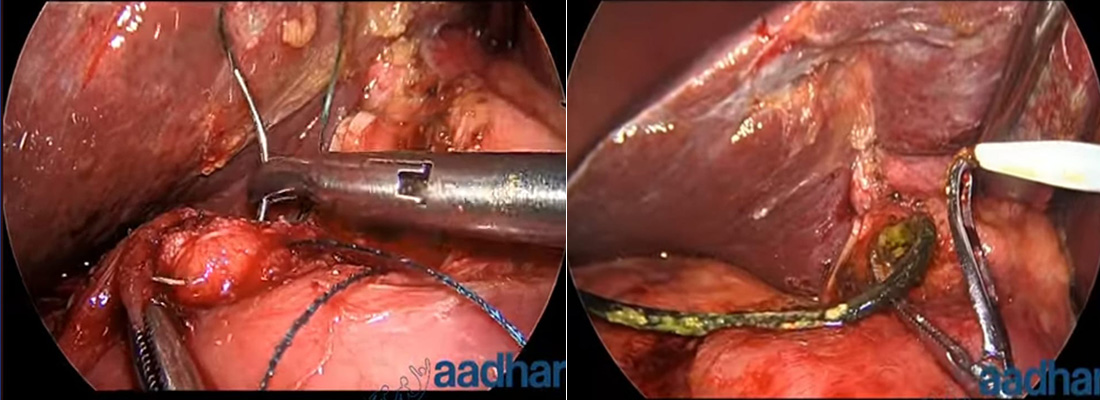
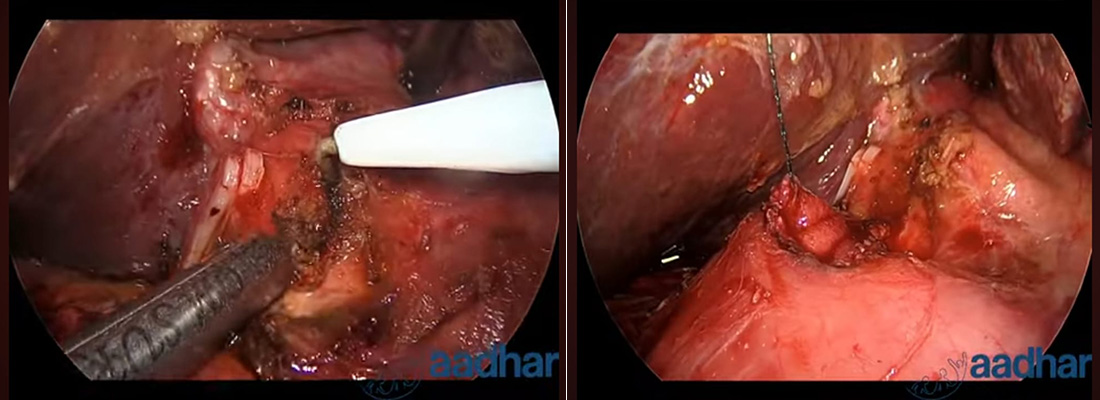
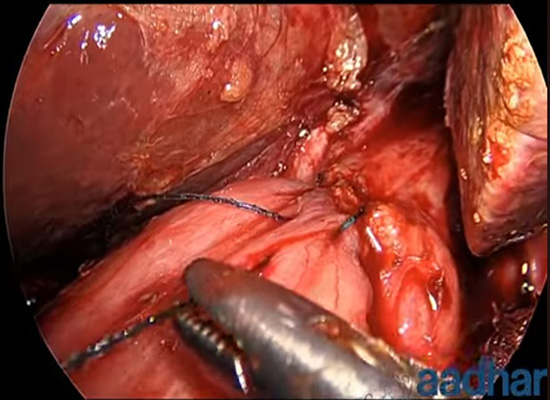
The patient underwent laparoscopic common bile duct (CBD) exploration with previous stent removal and stone retrieval on 03/07/2026. On postoperative day (POD) 1, significant bleeding was noted through the abdominal drain, necessitating emergency re-exploration on 04/07/2026 for hemostasis and gross hemoperitoneum was notes with clots. All the clots and blood aspirated and wash done , no active source of bleeding noted. Following surgery, she was managed in the intensive care unit with close monitoring and supportive care.
On POD 3, the patient developed malena with a progressive fall in hemoglobin levels. In view of ongoing gastrointestinal bleeding, CT angiography followed by digital subtraction angiography (DSA) was performed. The bleeding source was not identified, gastroduodenal artery prophylactical coil embolization was performed by the interventional cardiology team, achieving complete hemostasis.
Following embolization, the patient’s hemodynamic status stabilized, melena resolved, hemoglobin remained stable, and she showed gradual clinical improvement. She was started on oral feeds, mobilized, and discharged in stable condition with appropriate follow-up advice.